Name
*
E-mail Address:
*
Telephone
*
Date of Birth
*
Smoking Status
*
Smoker
Non-smoker
Amount of Coverage
*
$10,000
$20,000
$30,000
Gender
*
Male
Female
In the past two years, have you had any application for life, disability or critical illness insurance declined, postponed, cancelled, rescinded, rated, or modified for medical reason?
*
Yes
No
Within the past ten years, have you had any: abnormal diagnostic test results, including mammograms, PAP tests or abnormal PSA test for prostate cancer?
*
Yes
No
In the past 10 years have you consulted a physician, recieved treatment, advice or been prescribed medication for tumor, polyps, chest pain, palpitations, CVA, TIA, diabetes, kidney disease, hepatitis, or for any disorder of the liver or colon, AIDS or positive HIV test, angina or heart attack?
*
Yes
No
Are you aware of any symptoms or complaints regarding your health for which you have not yet consulted a physician or recieved treatment?
*
Yes
No
Have you been advised to have further examination, diagnostic testing, treatment or surgery that has not yet been scheduled or completed?
*
Yes
No
In the past 5 years, have you used any narcotics, cocaine, or other illegal drugs?
*
Yes
No
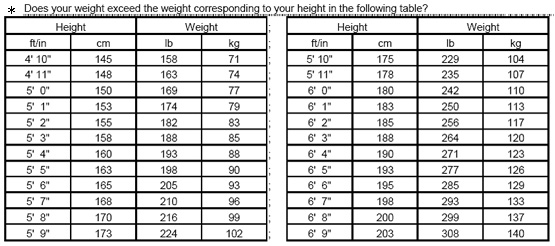
Does your weight exceed the weight corrosponding to your height in the table below?
*
Yes
No
Best time to call
*
8:00am
9:00am
10:00am
11:00am
12:00pm
1:00pm
2:00pm
3:00pm
4:00pm
5:00pm
6:00pm
7:00pm
Best days to call
*
Monday
Tuesday
Wednesday
Thursday
Friday
Saturday
Sunday
*
Required
Create Email Forms